I wanted to check if this knot has already been described. Adding an extra wrap of the suture around itself at the end of tying a double constrictor increases resistance to slippage about 50%, as measured by a tensiometer. I am thinking about including it in my book on advanced surgical knot tying as a way of securing a drain. A triple constrictor adds little, as the first and third wrap press down on the underlying wrap the same as a double constrictor and the second loop adds little (due to capstan effect). Thanks.
Good day Isleofgough.
The only thought I have on this is the fiddly-ness of drawing it all up tightly. I have no surgery experience and have a hard time imagining using small sutures in the environment it will be used.
Shouldn’t a single wrap Constrictor, with your extra wrapped working end suffice?
It could be that doing some wraps before the Constrictor might do a better job of tying off/stemming flow. (?)
SS
SS: you are correct that a single wrap Constrictor is adequate for securing a blood vessel. A slipped Granny followed by square knots is also reliable and easy to tie. I wouldn’t recommend a double constrictor for tying a blood vessel with fine suture, for the reason you mentioned.
Drains/tubes/IV lines are a different matter, where slipping longitudinally through the loop can be an issue. Tying down too tightly can also crimp the tube. Drains and tubes tend to be slippery and the suture itself is like fishing line. Multiple wraps don’t really help. For example, if one did ten wraps around the tube with the suture, the tension in the middle (between the 5th and 6th wraps) would be very low. One can think of it as a double capstan. The modification of the double constrictor was compared with the standard double constrictor by placing a tensiometer on the two loops at the opposite side of the tube to see how much tension was needed before slippage. It was about 50% more.
Ahh, my misunderstanding of that application.
IMO, the increased resistance to slipping on the tube might be the Knuckle formed at the extra wrap under the overlying turns. In essence, the tube is locally deformed and pushed into that spot, as well as giving the overlying wraps more to constrict.
As far as if this knot has been described, I can’t think of or remember (!) it in literature. But I have tied similar tangles, even reeving the working end through the hitch. Ends up looking like a messy Turks head knot. ![]()
ss
What software are you using to create those images? They are very nice.
I use Houdini Indie to do the illustrations, but any 3D program would work. Basically one sweeps a circle along a curve, adds texture and lighting and a camera. I chose Houdini as it is cheaper (free for the Apprentice version) and allows me to create a few points and have the program interpolate between them.
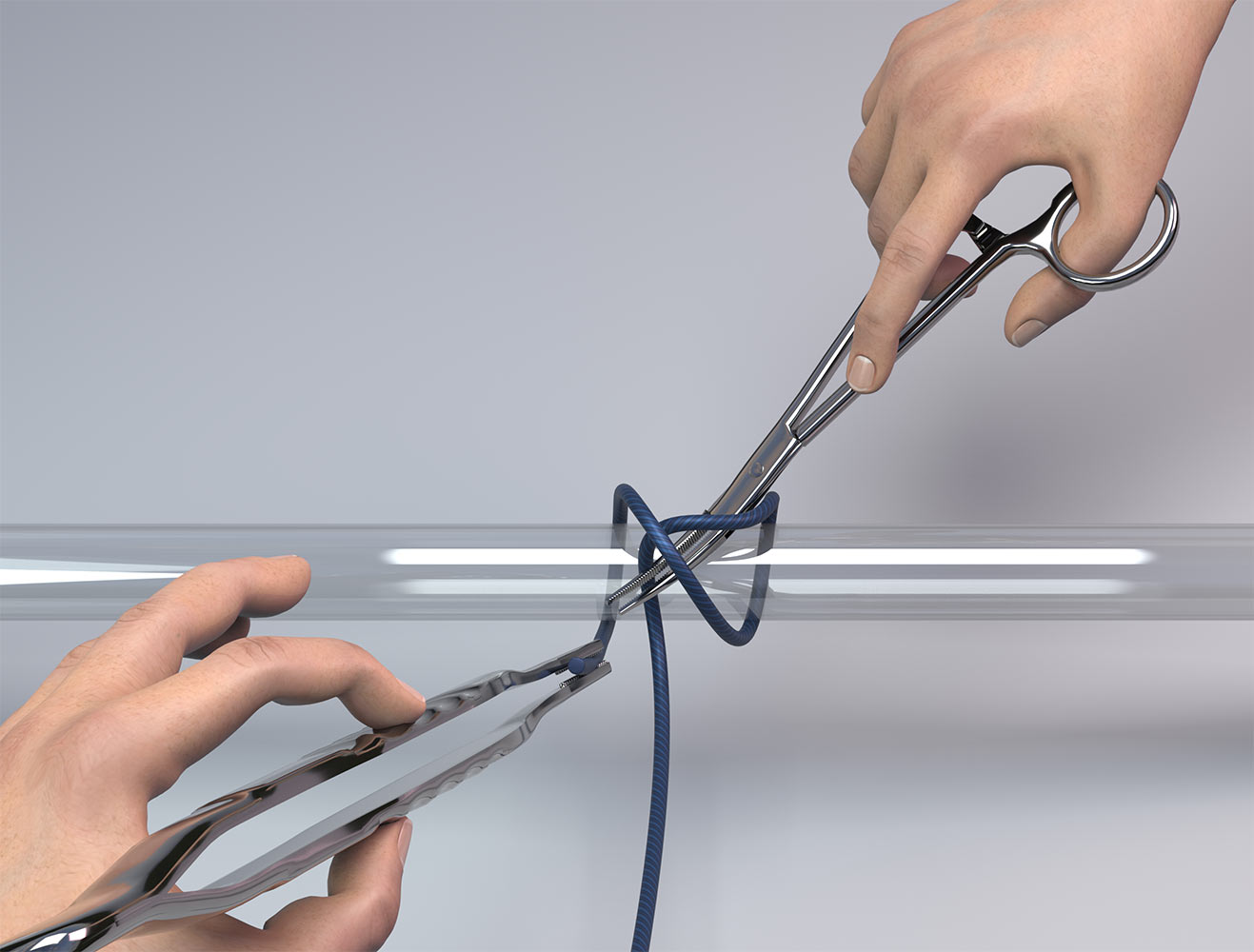
Here is how a regular constrictor would be tied to secure a blood vessel.
How does this tensiometer work, exactly?
A triple constrictor adds little, as the first and third wrap press down on the underlying wrap the same as a double constrictor and the second loop adds little (due to capstan effect).The more turns there are, the more tension must *travel* in order to make the binding area tight --for the [i]constrictor[/i], that's 360deg roughly, and more wraps will as noted suffer loss of tension via friction.
How about this : tie a slipped (singly) constrictor
and reeve the unslipped tail through the slip-bight
of the other, then draw the other tight down upon it.
(There is sometimes a tendency for the latter action
of tightening the slip-bight to loosen the base knot,
alas.)
Alternatively, one can follow the mistaken direction some
old knots book authors did in trying to make visual sense
of some cryptic words --misworded/omitted than imagined–
by tying off the tails with a simple “throw”/overhand crossing,
or even surgeon-ize that!?
A concern of extra crosses of the ends
is that they perforce are further deviated
from a tangential relation to the tied-to object
(e.g., with perfect tangent point say at 12:00,
they end up pulling away from the surface
more nearly at 10: & 2:00, and some of the
tightening pull goes to pressing upwards
into crossing wraps.
–dl*
The tensiometer is just a spring system that measures tension pulled on the two loops at the opposite side from the overhand or surgical throw (6:00 position). One can pull on it until there is slippage and test the difference between a standard double constrictor and the surgeon’s modification. I tested it with 2-o monocryl suture, which is similar to fishing line.
It may be that the double constrictor spreads the tension over both wraps a bit better than the single constrictor, avoiding the issue you mention of the wraps being at the 10 and 2:00 positions, rather than 12:00. In any event, for most suture and drains, the wraps will be closer to 11:30 and 12:30 positions, since suture is pretty fine.
Re the tensiometer, I’m just unsure of how well it
really is measuring vulnerability to slippage; there
might be some over-time loosening not seen in a
one-time loading!?
In any case, IMO if one can arrange to further
anchor one end of the constrictor with some
U-tuck (i.e., tucking a tail after making a U-turn),
it should be highly unlikely to gradually slip out,
and I think that with one tail unslipping, the knot
will well enough stem slippage of the other --that
there is generally needed some sympathetic
slippage in both … .
Or one might endeavor to set snug an overhand
stopper knot against the constrictor --though
I admit to finding this not all so easily done, when
I’m tying whippings with small stuff : one can get
the stopper pretty close, but “snug” takes some
extra & awkward tying. Closing with one bight-end
to draw down upon the opposite tail seems surest.
–dl*
Thank you for posting your surgical question in this forum Isleofgough.
Some questions if I may:
What length of time must this hitch remain effective?
That is, for what length of time is the hitch intended to be employed in its role?
Is the hitch intended to be employed only for a brief interval of time?
I’m guessing that any employed hitches/knots aren’t intended to be permanent (eg they naturally dissolve over time)?
Are there any mechanical stresses acting to influence the security of the hitch during the time frame in which it is employed?
Do you need to achieve the smallest possible ‘footprint’ with knots/hitches employed in surgical procedures?
By ‘footprint’ - I am referring to the bulk/volume of the hitch - and if too large a footprint, would this have an adverse/negative impact?
Is complexity in tying balanced against the desired effectiveness of the hitch/knot? I presume that you wish to avoid overly complex knot structures - and that you are seeking to employ the least complexity to achieve the desired objective?
The questions about surgical knots in general are good ones. Most surgical knots originated from when suture was composed of natural materials (cotton, silk, intestine, or even wire). Most modern sutures are monofilament, like fishing line, and may or may not dissolve over time. Monofilament sutures are less reactive (less scarring and inflammation), more resistant to infection, cause less sawing through tissue, etc. But knot techniques have changed little. It is a little like a fisherman who ties on the line with a lot of square knots.
The choice of suture and knot depends on a lot of conflicting factors: ease of tying, knot security, ability to tie down tightly, cyclic loading, knot profile, resistance to breaking, etc. Most surgical knots are not tied correctly. Look at the knots tied at your next emergency room laceration repair with a magnifying glass and you will see. A study out of the Mayo Clinic found that about 80% of knots were tied wrong. Howard Taylor and Alan Grogono suggested that the constrictor knot was the best knot for thing off blood vessels (Ann R Coll Surg Engl. 2014 Mar;96(2):101-5. “The constrictor knot is the best ligature”).
In Ashley’s book of knots, he states that Dr. Mayo used granny knots, and Mr. Ashley had to teach surgeon’s to use square knots instead. Personally, I feel Dr. Mayo was correct and Ashley, incorrect. The first two knots are often tied down as a slip knot to secure the blood vessel or appose the tissue. A slipped Granny slides down as a clove hitch, while a slipped square knot slides down as a cow hitch. The Granny slip resists back slipping better. Of course additional flat knots are needed at that point for security. The problem is that 7 or 8 flat knots is needed. That does create a bulky knot. Sometimes that does not matter, but in shoulder arthroscopy, a bulky knot is bad. For shoulder arthroscopy, self locking knots are sometimes used (similar to the the slip knot->cowboy bowline), but these loosen a bit during tying. Too loose is bad (more breakage). Too tight is bad (causes tissue to die and then falls out). Most of the time, picking the best knot is a compromise in which factor you want and what you are willing to deal with.
Isleofgough:
In reading your last post, I am left wondering if your references to ‘slipped’ are in fact a noose?
The term ‘slipped’ has a certain meaning in knotting. A knot that is ‘slipped’ can be easily/rapidly untied by pulling on a tail segment.
Also, it appears that the majority of your hitches have single leg loading profile. Meaning that your hitches are tied from a linear, open ended length of cord/material. This is in contrast to tying a hitch from a circle (ie round sling). For example, #1763 Prusik hitch is tied from a circle - and thus has dual leg loading. In contrast a Blakes hitch is tied from a linear open ended length of cord and has single leg loading profile.
And, they appear to be loaded in one direction only; uni-axial loading (ie there is one SPart and one tail). Rare to see biaxial loading profile?
For example, the constrictor hitch can be biaxially loaded (2 SParts) or uni-axially loaded (1 SPart).
I may be using the term “slipped” incorrectly, but that is how it is usually used in surgery. Yes, it is a noose, not a a slip loop to undo a knot.
Both the double constrictor and single constrictor used in surgery have biaxial loading. In the case of tying in a tube, both ends are tied under the drain through the skin, so tension pulls on both ends. A single constrictor ligation of a vessel also has biaxial loading. The only cases of uniaxial loading are when a running suture is done. Many incorrectly tie the initial knot down flat, but that actually increases the chance of breakage. Just tying as a noose, though, can over tighten tissue leading to damage. A common way of avoiding that is to use a Revo knot (one reversed half hitch somewhere in the knot).
The advantage to tying a granny knot and then converting it to a noose is that it doesn’t back slip during the creation of the knot. It is generally impossible to convert any noose/slipped knot back to a flat knot after tying in surgery, so flat knots are added to secure the noose. There are other ways of securely tying, such as the Mayo Clinic TSOL knot, which basically is a European death knot with a square knot tied on the ends to prevent loosening. The problem is that without clamping the suture (a bad thing), it is very difficult to get tight, though it is very secure.
We do have a Blake’s hitch type knot that is useful in laparoscopic surgery (though it is created to reduce widening of the loop, which is opposite the forces for which a Blake’s hitch or Prussik are used), called the Melzer:
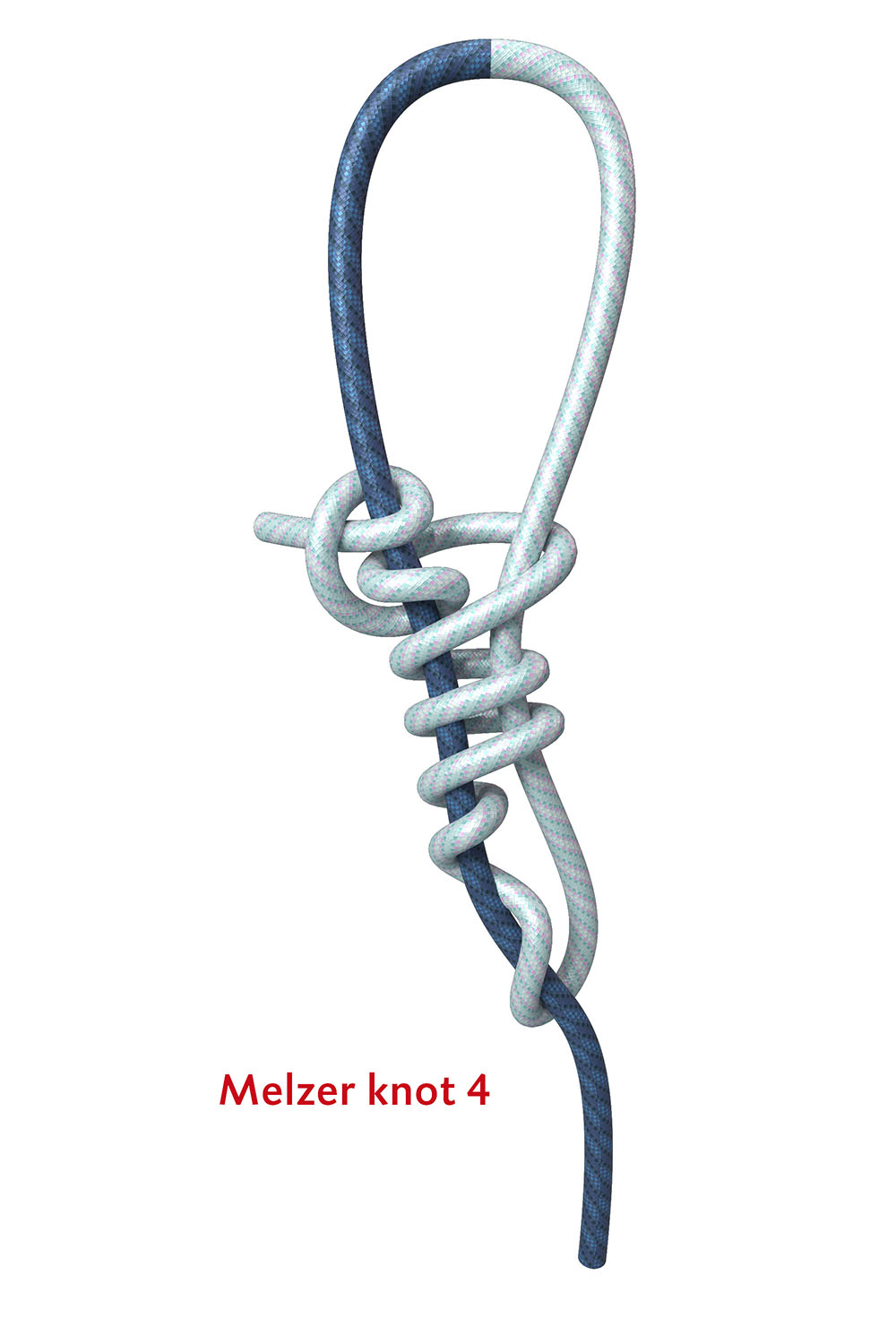
Although it is a bit off topic, the Melzer knot actually works best as drawn above, rather than with a clove hitch for the terminal wraps. There are two other knots that are used all the time in surgery, with similar desired properties: a zip tie equivalent. Neither have names, and they both depend on perfect dressing of the knots. I would not be surprised if the company that makes the pretied version uses a drop of superglue to keep the dressing. They are described in the patent: http://www.google.com/patents/EP0477020A1?cl=en
I have never seen any discussion of their properties, but they are used all over the world every day.
For locking knots, there are over a dozen which are not even described in Ashley’s book of knots: SMC, Dines, Outback, Pretzel, Weston, West Point, Gea, Mishra 1 and 2, Duncan, Tayside, Giant knot, and others.

I see exactly a clove h. in the tail end of this
knotting above!?
As a general tactic, how might this work:
- form a broad loop in the pulled-on part,
and - knot variously around this, SUCH THAT
- this knotting of the “working” end will enable
initial tightening of the knot as desired,
AND THEN - the tail end can be drawn through the
“1” loop which is then drawn down upon
it to nip/hold it.
In short, IMO this is the point of the Stevedore knot
–a stopper knot knob that is hardly much bulkier
than simpler knots (for pulling through a hole),
but whose wraps can provide gripping against
the straight-through-tuns SPart whose turn
nips the tail : with tight wraps the SPart’s hard
nip on the tail (which terminates those wraps)
can be sustained.
SO, in general outline, this is a tactic to try to use
for designing some of these surgical knots, it seems.
(A general way to form a stopper is to fashion
some noose and then noose the tail
–Ashley’s stopper does this from a slip knot.)
Oh, the breadth of my conjectured initial loop
above is to leave ample real estate on that line
for gripping and pulling and setting the knot
(without tightening the loop, until ready).
–dl*
My diagram may be a bit misleading, as I show the tail off to the left, but if you look closely, it is a cow hitch in my illustration. I think it works better as a cow hitch as it was originally described: see https://www.laparoscopyhospital.com/extracorporael_knot.html and https://books.google.com/books?id=0PsEGivLBAwC&pg=PA34&lpg=PA34&dq=melzer+knot+1991&source=bl&ots=WjAmckNuIj&sig=ACfU3U1ygvf2cMCY4WQnB7jCeP8G84gekg&hl=en&sa=X&ved=2ahUKEwit7_yk0-DkAhXFpZ4KHXnBCW04ChDoATAAegQIBxAB#v=onepage&q=melzer%20knot%201991&f=false
I read your paper on extracorporial knots- very interesting.
Some of your terminology could (in my view) be aligned with the concept of chirality (handedness).
For example; in the attached diagram, one loop has Z chirality and the other loop has S chirality.
This is an improvement over descriptors such as ‘under-over’ and ‘over-under’ which could be misinterpreted if the reference frame is not clear.
I am also curious as to how some of your ‘binder’ hitches (eg Constrictor) are biaxilly loaded?
I understand this to mean that both SParts are loaded equally.
In your surgical contexts, maybe each SPart is not under an identical loading profile? Or is there mirrored (identical) loading on each SPart?
I referenced the paper (which is not mine) just to show the configuration of the Melzer knot. It is an interesting paper, and relatively little has been written comparing various knots where the tension in tying can only be in the directions away and towards yourself (which is the common denominator of extracorporeal knots). These knots are tied outside the body and slid down through a tube into the body to secure a structure. Most of them are what you would call a noose, but a few lock into place, or added half hitches are placed to prevent unslipping. Lots of institutions and surgeons have given their own names to these types of knots, and most have little advantages over previously described knots (like the West Point knot, Wiese, Mishra, etc.). You are right that the terminology can be confusing. I changed the term “slip knot” in my book to “noose” based on the comments on this thread. What you describe as chirality reminds me of enantiomers in organic chemistry. They can be difficult to depict with a two dimentional diagram.
I personally only teach one knot that is similar to a zip tie: the Melzer. I show only one locking knot: the Outback knot. For nooses, I describe the differences between a converted square and granny knot as well as show how to tie a Nicky knot (which is a noose converted from a granny version of a surgeon’s knot). The other knots don’t have much to offer over these few.
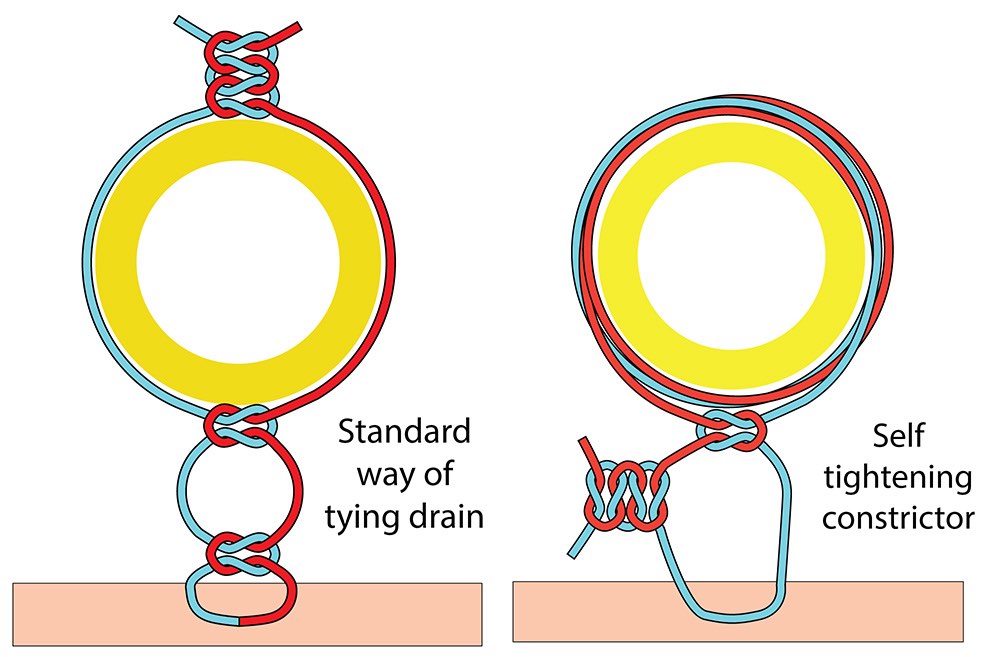
But back to biaxial loading, a drain is tied to the skin, but in such a way that the skin is not pinched and the drain doesn’t lie immediately adjacent to the tube. The advantage of a constrictor or double constrictor over the usual way of tying this knot is that it is self tightening and functions a bit like a Prussik to prevent sliding of the tube. What I proposed is tying the constrictor knot first around the tube and then suturing with a loose knot to the skin. There will be biaxial loading, but since the double constrictor is not symmetric, it will tighten a bit more in response to tugging on one side versus the other. The standard way of tying in a tube looks somewhat like this:
Except that the images are wrongly labelled :
the “Z” & “S” belong on each other’s image.
(Looking down at the respective turns, the
“Z” should --like Z-laid rope-- turn to the right,
and so on.)
–dl*
Except that the images are wrongly labelled : the "Z" & "S" belong on each other's image.
Are you sure?